A Tale of Two Covers — How the Manchurian Plague of 1910 – 11 Contributed to the Global History of Medical Equipment
Written by Xiaomeng Liu
Published on 08/11/2021
Masks have never been more symbolic and integral to global public health. In 2020, the COVID-19 outbreak and subsequent full-fledged pandemic caused demands for masks (especially N95 and surgical masks) across the world to rise to unprecedented levels. Even though at first there were controversies surrounding whether or not masks were effective for curbing the spread of the virus, most countries soon resorted to mandating that all citizens wear masks in public, which quickly led to a mask shortage and caused mass panic. As the use of surgical and N95 masks spread, with the masks themselves losing their prestige as a medical-grade equipment and becoming a mere everyday object, a great deal of discussions were induced not only within academic circles but also among the general public. A wave of rediscovery and retelling of the history of masks has since been seen on social media, in the media, as well as academic journals and conferences.[1]
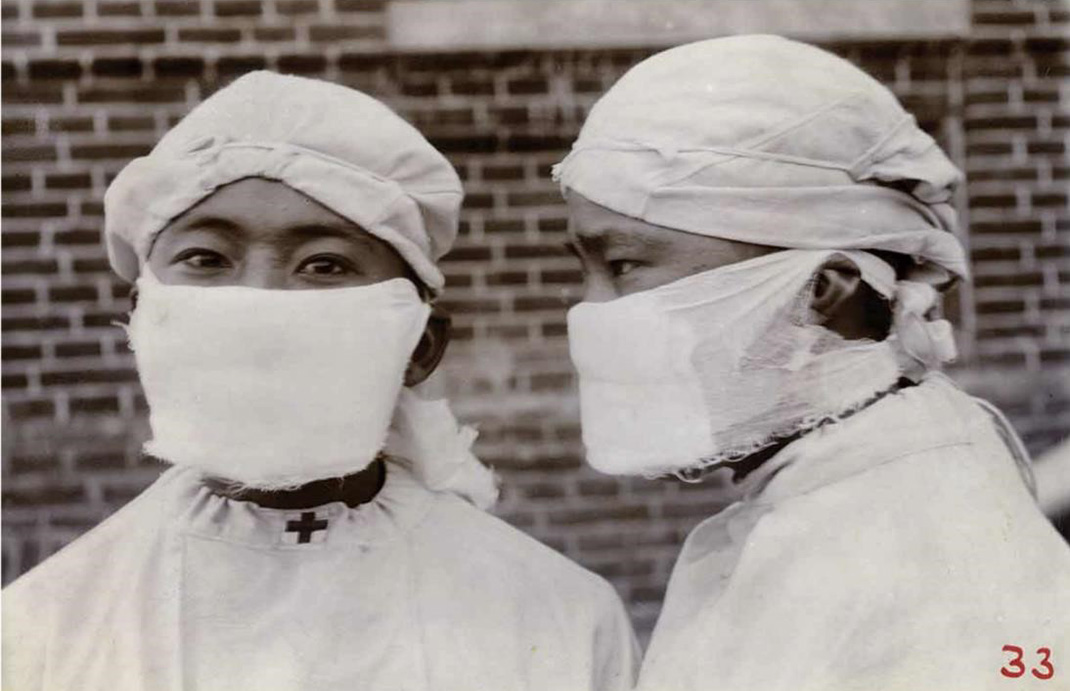
Figure 1, which is a century-old photograph, has made frequent appearances in articles recounting the history of masks. In the photo are two young men in full medical protective gear. The man on the left has a red cross on his collar, and, from that, one could guess that they are either doctors, public health workers, or paramedical personnel. The man on the left faces the camera; the other shows his side profile. They each wear a large, thick mask made of gauze. This photo also appears in Wu Lien-teh’s North Manchurian Plague Prevention Service Reports (1918 – 1922) with the caption “How antiplague masks are worn.” This caption is telling: the photo was not intended as a record of public health workers fighting the Manchurian Plague; instead, it was meant to demonstrate how the masks should be worn.
Until recently, this photo did not stand out from photos that documented the 1910 – 11 Manchurian Plague, suggesting that the practice of wearing masks was of lesser importance than other more stringent public health measures undertaken during the plague, including lockdowns of sizable areas, house-to-house inspection, strict quarantine, and mass cremation. Today, however, as masks became an important object during COVID-19, scholars have started to rethink the seemingly ordinary object and its historical importance during the Manchurian Plague.
In 2020, renowned medical journal The Lancet published an article on the history of medical masks. In its rather Eurocentric narrative, only one sentence mentions the Manchurian plague and its place in the history of medical masks,[2] but as this essay attempts to show, a certain mask invented during the Manchurian Plague turns out to represent an important phase in the history of medical masks and personal protective equipment against bacteria and viruses.[3] The mask, known as “Wu’s mask,” was allegedly invented by Wu Lien-teh. A hagiography of Wu now also spreads across Chinese social media, hailing him not only as a hero who successfully controlled the deadly plague in Manchuria, but also as a talented young scientist who discovered the airborne transmission of Yersinia pestis, and subsequently devising what would become a widely used piece of protective equipment. However, as much as Wu’s mask is a piece of ingenuity it is also shrouded in myths. Based on two recent in-depth research studies on this subject, we have finally pieced together a clearer picture of the mask and re-evaluated its significance in the global history of medical masks.
Even though masks have become a commonsensical thing nowadays, back in the 19th and early 20th century, they had neither a unified form nor even a name. Many researchers now trace the origin of modern medical masks back to either the respirator invented by British surgeon Julius Jeffreys in 1836, or the surgical mask introduced by Polish surgeon Jan Mikulicz-Radecki in 1897, but these narratives have neglected a technicality: after the introduction of germ theory and droplet infection in the mid-19th century, many doctors and public health experts began to use devices similar to Jeffreys’ respirator, but under an entirely different logic — Jeffrey’s respirator functioned by warming the air inhaled by a patient with a respiratory disease, while the other similar devices after the mid-19th century used them as a protective gear to filter out pathogens. Moreover, although they shared similar appearances, they began to be fabricated with new materials that would repurpose them more for general public health than for relieving specific patients’ ordeal. In some respirators, charcoal was used in the filter. Others used cotton-wool. Some even added antiseptic agents like carbolic acid and creosote.
The Manchurian Plague — one of the deadliest epidemics in recorded modern history — was, unlike other major historical outbreaks of the plague that happened in Europe, Hong Kong, and India, predominantly of the pneumonic type (which means that the patients contracted the bacteria mainly via airborne transmission rather than through agents such as rats and fleas). To protect against and combat a pneumonic plague, British, German, Japanese experts and authorities had called the respirator essential.
There was a geopolitical complexity to the Manchurian Plague: Manchuria was home of the Manchus, the ruling ethnic group of the Qing empire. However, since the late 19th century, the Russian and Japanese colonial powers had gradually extended their influence into Manchuria. For fear that the Russian and Japanese would further encroach on Manchuria’s sovereignty during their effort to contain the plague, two months into the epidemic, the weakening Qing state took action in Fuchiatien and named Dr. Wu Lien-teh, a Cambridge-trained Malaysian-Chinese doctor, chief medical officer and sent him to Harbin, the epicenter of the plague.

{kind=link}
Arriving in Harbin in the cold of the winter of 1910, Wu observed the protective gear used by public health workers and saw two types of masks, one being “a readymade wire-meshed frame covered with black muslin and adjustable to the human mouth and nose,” the other “a soft piece of surgical gauze and cotton contrivance” covering the lower part of the face. The first type resembled the respirators used by the Europeans and Japanese during the plague; the latter, mostly referred to as “gauze and cotton-wool mask,” was self-made by the Chinese, and, though simpler, was perhaps more popular among the Chinese.
The Chinese in Harbin did not have a sufficient supply of readymade respirators, many of them therefore fashioned their own protective gear. Because they had already known with certainty, through two doctors (before Wu’s arrival), that it was a plague of the lungs, the response teams knew to specifically guard their airways and orifices against coming into contact with the airborne pathogens. It is said that the rat-control teams even plugged their nostrils and mouths with cotton.[4]
Clearly, the gauze and cotton-wool masks — which soon after Wu’s arrival in Harbin were worn by most Chinese and even Russian plague-control personnel — became the prototype for the subsequent “Wu’s mask,” which was soon deployed to Fengtian (or Mukden, present-day Shenyang). An American doctor there noticed the masks and called them “Mukden masks.” Therefore, though these masks were credited to Wu, clearly he was not the inventor. In fact, at the International Plague Conference held at Mukden, a Chinese medical officer called Fang Qin (1884–?) presented the mask not with Wu’s name but as a resulting invention of the Harbin Chinese plague-control team’s collective effort. The following is a detailed description of the anti-plague mask:
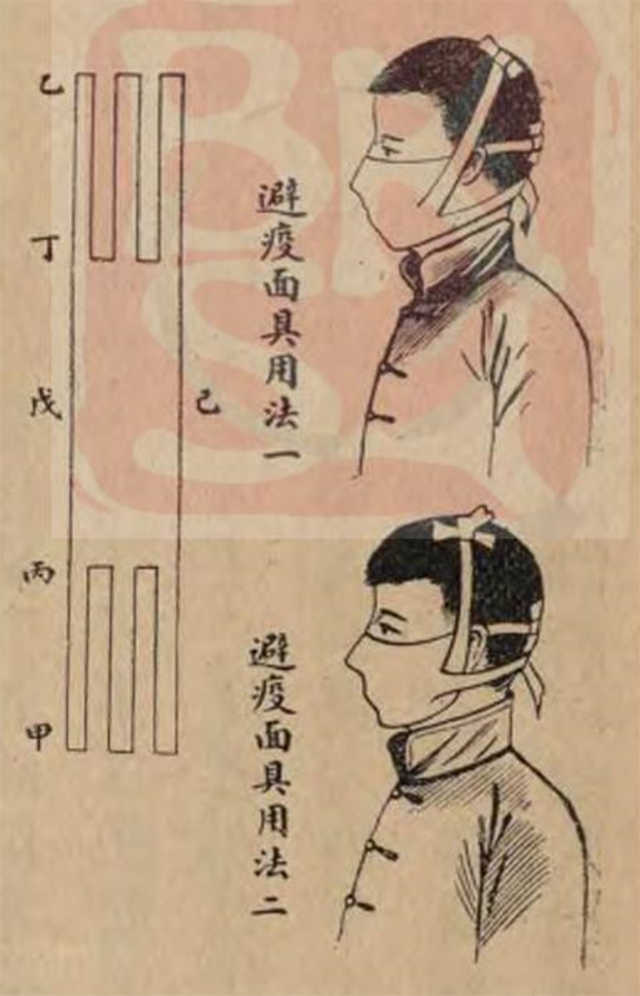
[It] consists of two layers of gauze enclosing a flat oblong piece of absorbent cotton 6 inches by 4 inches. It can be easily made by cutting the usual surgical gauze (9 inches wide), as supplied from the shops, into strips, each measuring 3 feet in length. Each strip is then doubled lengthwise so as to contain in the middle a flat piece of cotton wool measuring 4 inches by 6 inches. At either end of the gauze two cuts, each measuring 15 inches, are made. Thus turning the pad into a three-tail gauze bandage, with the central piece of wool for covering the respiratory entrance. The upper tail of one side should be passed round the side of the head above the ear and tied to the other corresponding tail. The lowermost tail should in a similar manner be passed under the ear and tied to the one on the other side, while the middle tail should be passed over the crown of the head, so as to fix the pad and prevent it from slipping down the neck.[5]
The design of the mask seems primitive; they certainly were not as sophisticated as today’s surgical masks. Even though the gauze covered a larger part of the face than contemporary masks, it would be reasonable to question whether a two-layer gauze with cotton inside could really block the transmission of pathogens.
In fact, other more “advanced” mask-like equipment also appeared during the plague. For example, the Japanese colonial authority in South Manchuria required the use of conventional but supposedly more advanced respirators in the army. Besides these respirators which covered both the nose and the mouth, the Japanese also had what was called the “Kanata style respirator.” In addition to their metal frame and replaceable cloth, these respirators were attached with goggles on top.
Meanwhile, a British company dispatched a batch of masks that covered the whole head with glass goggles secured in place — it was French specialist Charles Broquet who thought it necessary to protect the eyes from exposure to pathogens. As much as Broquet was questioning the effectiveness of using cotton and wool pads, he was actually attempting to promote his own design — a mask with full headgear and mica goggles.


The gauze and cotton-wool mask was indeed a more modest but practical design; the aforementioned Chinese medical officer Fang named “simplicity of construction” and “cheapness” as its most significant advantages. As there were around 11,000 plague-control personnel (excluding street sanitary workers, policemen, and porters for carrying corpses), it would have been a logistical nightmare to ensure a sufficient supply of masks for every one of them, not to mention for the vast number of patients as well. A gauze and cotton-wool mask only cost about 1 cent to make, compared to the Japanese respirator’s 12 cents. Moreover, the masks required neither factories nor professional workers to manufacture; anyone could make one at home.
In addition to being economical and practical, these masks also suited the weather of Manchuria. As the plague control team had to work outdoors in the cold winter, if one wore a headgear mask or separate googles and mask, the person’s own breath, which would be much warmer than the ambient air, would easily cause the googles to fog up and obstruct the person’s vision. The gauze and cottonwool mask would not have this problem, though it would still keep the face warm while outside. Of course, this mask did not have a snug fit on the face, which could reduce its effectiveness in blocking bacteria, but it nonetheless found a middle ground between medical efficacy and practicality. At the very least, one could breathe more easily through the mask than the respirator. In light of the recent COVID-19 pandemic, one could not help but notice: while the N95 mask was more effective in filtering out the virus, it was indeed the surgical mask that was more economical and convenient, eventually becoming the more popular choice of protection.
The International Plague Conference that took place in April 1911 in Mukden gave its approval and recognition to the gauze and cotton-wool mask, citing: “The best form of mask is a simple, three-tailed, gauze and cotton-wool pad, which should be destroyed, or disinfected, after each tour of duty.” However, only a few months later, Richard P. Strong and Oscar Teague, two U.S. epidemiologists who participated in the effort to contain the Manchurian Plague, somewhat refuted the International Plague Conference’s verdict. Upon returning to the Philippines, they conducted an experiment to show that salt solution sprays with Bacillus prodigious could penetrate the gauze and cottonwool mask, but they nevertheless conceded that in times of a plague, this form of mask would still be efficacious — to a point — in blocking contagions.
For Wu, on the other hand, he would not turn his back on his much acclaimed mask simply because someone had filed a critical report even if it were scientific. His mask would continue to be used in epidemic control in China. It was not until early in the 1920s when a small plague struck Manchuria once more that Wu started to devise his own experiments to validate his mask, and though not fully successful in obtaining the confirmation that he was looking for, he insisted on its effectiveness. Wu also began to promote the design of the mask on different occasions including in his own publications. In several influential works on the Manchurian Plague, Wu and his assistants made explicit claims that the mask was indeed introduced by Wu, thereby contributing to giving the mask the name “Wu’s mask.” Nevertheless, even had he not been the mask’s originator, Wu did subsequently improve its design. As shown in the first picture in this essay, the masks worn by the two men had two tails rather than the three that was described by the International Plague Conference. This was a major change introduced in the 1920s that was certainly attributable to Wu.
Wu’s mask has three important legacies, particularly in terms of how it influenced the development of medical masks in the 20th century. First, the disappearance of a metal frame made the mask more convenient to wear than its predecessors (i.e., respirators). This form was soon adopted by the Western world during the Spanish flu in 1918, and the metal frame is completely absent in today’s mainstream masks. Second, the International Plague Conference established a significant principle concerning the usage of masks (which has become commonsensical for us today): masks should be used as a physical barrier against bacteria without any chemical disinfectant. Third, to quote the Report of the International Plague Conference again: “The best form of mask is a simple, three-tailed, gauze and cotton-wool pad, which should be destroyed, or disinfected, after each tour of duty” — in other words, masks should be disposed of after a single day of use. This suggests that today’s throwaway culture of masks (as proposed by Bruno J. Strasser and Thomas Schlich in their 2020 Lancet essay) may have had a much earlier origin.
Footnotes
- This essay is based on the materials and insights of two ingenious research published recently in Chinese: 1. Zhang Meng 張蒙, “wushi kouzhao de youlai” 伍氏口罩的由來 [Origin of Wu’s mask], Jindai shi yanjiu 近代史研究 [Modern Chinese history studies] no. 2 (2021): 148–159; and 2. Wang Yumeng 王雨濛, “Gengxu shuyi yu wushi kouzhao de dansheng” 庚戌鼠疫與伍氏口罩的誕生 [], Nankai xuebao 南開學報 [Journal of Nankai University], no. 4 (2021): 71–85. The first article has an English version available: Zhang Meng, “From respirator to Wu’s mask: the transition of personal protective equipment in the Manchurian plague,” Journal of Modern Chinese History 14 (2021): 221–239. I also thank Zhang Meng for providing me with the historical pictures contained in his essay.
- Bruno J. Strasser and Thomas Schlich, “The Art of Medicine: A History of the Medical Mask and the Rise of Throwaway Culture,” The Lancet 396 (2020): 19.
- Christos Lynteris, “Plague Masks: The Visual Emergence of Anti-Epidemic Personal Protection Equipment,” Medical Anthropology 37 (2018): 442–457. The author further elaborates on the significance of Wu’s mask in a interview, calling it “the first modern respirator,” and predecessor of the N95 mask, which is widely used during the COVID-19 pandemic. See “The untold origin story of the N95 mask,” https://www.fastcompany.com/90479846/the-untold-origin-story-ofthe-n95-mask (accessed on 1 November, 2021).
- Wu Lien-teh, Plague Fighter: The Autobiography of a Modern Chinese Physician (Cambridge: W. Heffer & Sons Ltd.), 8.
- Wu Lien-teh, Treatise on Pneumonic Plague (Geneva: League of Nations, 1926), 393–394.